
Hiatus Hernia
What is a hiatus hernia?
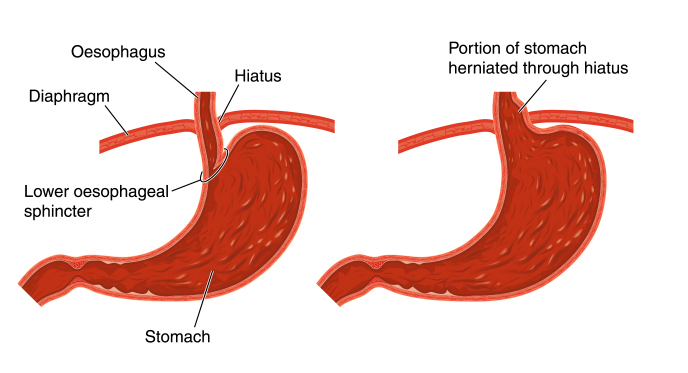
The stomach migrates into the chest through a weakness in the diaphragm (hiatus). Part or the whole of the stomach can then lie in the chest cavity. Small hiatus hernias (2-3cm) are very common and can be found in approximately 50% of individuals over the age of 50.
Why does it happen?
The diaphragm muscles, which surround the oesophagus, can weaken with time allowing the stomach to push into the chest. Once this happens, the pressure differences between the abdominal and chest cavities promotes acid reflux.
What symptoms do they cause?
Small hernias may not cause symptoms. When they do, the most common symptom is acid reflux, which is often controlled with simple medication. If surgery is required for reflux, then the hiatus hernia will be repaired at the same time.
Larger hernias can cause severe reflux, swallowing issues and chest or abdominal pain. Patients can report an inability to eat normal sized meals and may suffer from regurgitation. The stomach can intermittently rotate or twist resulting in severe pain. This is a surgical emergency.
When should I seek help?
How are they assessed?
Gastroscopy – is usually the first investigation to be performed for patients presenting with symptoms suggestive of a hiatus hernia.
Barium Swallow – This is an x-ray test performed whilst drinking contrast. It is painless and quick and gives useful information on the anatomy and size of the hernia.
CT Scan – The CT scan will assess the anatomy of the hernia and give more information about the size of the diaphragmatic defect.
Oesophageal Manometry – is often used to exclude other oesophageal motility disorders such as achalasia. Acid pH studies, either via a 24-hour catheter study or BRAVO, are generally used to quantify reflux in patients’ considering surgery.

How should it be managed?
How is the surgery performed?
It is a keyhole procedure. Five small cuts are made in the abdominal wall to allow passage of the instruments. The stomach is brought back down into the abdominal cavity and the diaphragmatic defect is repaired. The procedure normally takes a couple of hours. An anti-reflux procedure is also performed to help prevent post-operative reflux and to help fix the stomach in the abdominal cavity. This can take the form of a fundoplication or linx procedure.
More information on Laparoscopic Surgery
How effective is surgery?
Are there any risks?
Patients can suffer from gas bloating or increased flatulence (passing wind). This is due to the inability of air to escape past the new sphincter created to prevent reflux. This usually improves over time. Avoidance of fizzy drinks and certain foods may improve these symptoms. Some patients are unable to vomit, but this is not dangerous and complications from this are extremely rare. Temporary difficulty swallowing solid food can occur following anti-reflux surgery due to swelling around the oesophagus and the tighter valve resulting from the operation. This resolves over a short period of time and it is rarely an issue long-term. Some small risks that are present for any kind of surgery (e.g. wound infection) will be discussed during the consent process. Injury to the oesophagus or stomach during the procedure is an uncommon event, which may result in conversion to an open operation.
How long will it take to recover from the surgery?
Patients are fully mobile after surgery and can commence fluids immediately after. The procedure can be performed as a day-case or a one-night hospital stay. This is mainly to build confidence with oral intake after the surgery. The wound sites will have local anaesthetic injected into them at the time of surgery. This will wear off about 6 hours after the procedure. To stop the sites becoming sore you should take the regular painkillers as instructed. Shoulder tip pain is not uncommon and is due to gas underneath the diaphragm. This should not last longer than 24 hours. You will not be discharged until you are comfortable drinking. On discharge you should be independent and able to climb a flight of stairs. You can undertake any non-strenuous activity within two days of surgery. Avoid heavy lifting or strenuous activities for 6 weeks.
The post-operative dietary plan varies slightly by procedure. Following a fundoplication, patients build up steadily over some weeks from liquids to pureed food and then a soft diet before returning to normal eating. This can vary between individuals with swallowing difficulties prior to surgery a predictor of a slower progression after it. Following a Linx procedure, patients are encouraged to return to a soft diet on the day of the procedure as it is beneficial for the device to function (open and close) earlier.
Which medications will I require after surgery?
When can I return to work?
When can I drive?
Who do I contact if there are concerns?
The group practice telephone is answered in working hours and messages can be left out of hours. Any concerns will be relayed directly to the consultant surgeon on receipt. The hospital ward also provides a 24/7 means of contact. They will contact the consultant about any concerns and are able to give advice if required.
For more information on anti-reflux surgery in London, Hampshire or Surrey please contact us on davies@londonsurgicalgroup.co.uk